Mijn veulen heeft een standafwijking: wat nu?
Mijn veulen heeft een standafwijking: Wat nu?
The English version can be found below
Het veulenseizoen is weer volop aan de gang en de eerste veulens dartelen al vrolijk rond in de weide. Iedere fokker hoopt natuurlijk op een gezond en correct gebouwd veulen maar niet alle fokkers hebben dit geluk. Bij sommige veulens merkt de eigenaar, smid en/ of de dierenarts dat er iets afwijkend is met de stand van de hoef of het volledige been.
Het tijdig opmerken van een afwijking laat een snelle correctie toe indien nodig. Bij twijfel contacteert de eigenaar best de dierenarts/dierenkliniek om de stand van de benen van het veulen te laten controleren en op die manier tijdig de juiste behandeling toe te kunnen passen.
Beoordeling van de stand van de ledematen bij het veulen
De beoordeling van de stand van de ledematen bij het veulen wordt het best uitgevoerd op een harde, gelijkmatige ondergrond.
Hierbij bekijken we het veulen zowel stilstaand, waarbij getracht wordt het veulen zo vierkant mogelijk te positioneren, als in stap op de rechte lijn (figuur 1).

figuur 1: De beoordeling van de stand van de ledematen bij het stilstaande veulen
Bij de stilstaande beoordeling wordt het veulen bekeken vanuit de voorzijde voor de voorbenen en vanuit de achterzijde voor de achterbenen. Dit doen we best loodrecht op de voorknie respectievelijk sprong van het veulen. Op die manier kunnen we angulaire deformaties (O-benen of X-benen ) opsporen.
Er wordt gekeken of er een ‘denkbeeldige’ rechte lijn kan getrokken worden door het midden van de hoef, koot, kogel, voorknie/pijp en bovenbeen. Is dit het geval, dan zijn er geen angulaire deformaties aanwezig. Indien er een hoek zit in deze ‘denkbeeldige’ lijn dan wordt er gesproken van een varus (O-benen, linker paard op figuur 2) of valgus (X-benen, rechter paard op figuur 2). Vervolgens kan met behulp van radiografieën gekeken worden hoeveel graden de afwijking bedraagd en of chirurgische interventie noodzakelijk is.
 en x-benen (rechts)")
figuur 2: Een schets van een paard met O-benen (links) en x-benen (rechts)
Het veulen wordt beoordeeld van aan de zijkant om ‘flexural’ deformaties (buigpees retracties) op te sporen
Bij de ‘flexural’ afwijkingen zijn in het merendeel van de gevallen de buigpezen betrokken. Bij retractie van de buigers groeit het bot te snel in vergelijking met de pezen en trekt het gewricht in buiging (figuur 3a). Hyper extensie of overdreven gestrekt zijn van een gewricht komt meestal voor bij de geboorte van het veulen door laxiteit van de buigpezen ( figuur 3b)

 van zijn buigpezen")
Figuur 3a: Veulen dat op 2maand ouderdom plots op zijn teen begon te lopen links voor ten gevolge van een contractie van de diepe buigpees
Figuur 3b Pony veulen dat door zijn kogels zakt door een abnormale laxiteit (niet sterk genoeg zijn) van zijn buigpezen
Oorzaak van standafwijkingen bij veulens
Eenvoudigweg gezegd kunnen de oorzaken in 2 grote groepen opgedeeld worden:
1) Oorzaken die aanwezig zijn voor de geboorte.
Bijvoorbeeld : abnomale ligging in de baarmoeder, vroeggeboorte, ontsteking van de baarmoeder, ziekte van de merrie, hormonale- of nutritionale inbalans, onvolledige verbening van het bot, …
In dit geval wordt het veulen geboren met de afwijking.
2) Oorzaken die aanwezig zijn na de geboorte:
Bijvoorbeeld : niet-uitgebalanceerde voeding, trauma van de groeischijf, pijn (door trauma, een kneuzing, ‘hoefblein’,…) met secundaire retractie van de pezen, te snelle groei van de botten, infectie van de groeischijf, ongelijke belasting van de groeischijf, overbelasting van de groeischijf, …
In dit geval ontstaat de standafwijkingen in de eerste 6 tal maand na de geboorte.
Soorten standafwijkingen en hun behandeling
X en O benen vanaf de geboorte door onvollodige verbening van de botjes van de voorknie of sprong:
Bij te vroeg geboren veulens kan een O- of X-been onstaan doordat de kleine botjes in de voorknie of sprong onvoldoende verbeend zijn (figuur 4B). Het veulen gaat op deze fragiele botjes gaan lopen en drukt ze plat. Hierdoor zal er een abnormale stand ontstaan.
De behandeling bestaat uit een 2 tal weken stalrust in combinatie met een spalkverband. Eenmaal er voldoende verbening van deze botjes is opgetreden is het gevaar geweken.
Het proces van voldoende verbening wordt opgevolgd door radiografieën te nemen


figuur 4A: een radiografische opname van de normale verbening van de beentjes van de voorknie en figuur 4B een radiografische opname van een onvolledige verbening van de beentjes van de voorknie door een te vroeggeboorte.
Een andere oorzaak van O- of X-benen vanaf de geboorte is dat sommige veulens worden geboren met een O- of X-been door een foutieve ligging in de baarmoeder. Deze afwijkingen verdwijnen meestal spontaan in de eerste 4 levensweken en hebben geen behandeling nodig.
Door de kogels zakken vanaf de geboorte:
 van zijn buigpezen")
Figuur 5: Pony veulen dat door zijn kogels zakt door een abnormale laxiteit (niet sterk genoeg zijn) van zijn buigpezen
Dit probleem doet zich voor bij pasgeboren veulens en vooral in de kogels. Ze lopen op de achterzijde van de kogels (figuur 5)
Het gaat hier om een laxiteit van de pezen en gewrichtskapsel en in de meerheid van de gevallen lost het probleem zich zelf op in de loop van de volgende weken als het veulen groeit en sterker wordt.
De behandeling bestaat uit rust in een grote box en dagelijks gecontroleerde beweging (stappen naast de merrie) gedurende 15 minuten per dag om de spieren en de bijhorende structuren sterker te maken. Vrij weidebeloop wordt initieel afgeraden daar dit een overbelasting van de gewrichten kan veroorzaken.
Verbanden worden in dit geval afgeraden om dat deze de situatie kan verergeren.
X en O benen die ontstaan tijdens de groei van het veulen:


Figuur 6A: Links voor O-been door ongelijke groei ter hoogte van de groeiplaat van de kogel.
Figuur 6b: X-been links en rechts voor door ongelijke groei ter hoogte van de groeiplaat van de voorknieën
Deze ontstaan meestal de eerste weken/maand na de geboorte en een X-been is meer voorkomend dan een O-been.
Normaal groeit de groeiplaat in een bot over zijn gehele lengte gelijkmatig . In sommige veulens groeit echter de ene kant sneller dan de andere kant. Dit kan dan resulteren in een O-been (figuur 6A) of X-been (figuur 6B).
Erfelijkheid speelt hier ook een rol in.
Het bot heeft echter een mechanisme om deze ongelijke groei in bepaalde mate uit zichzelf te corrigeren. Operatie van een X-been is dus niet onmiddellijk nodig. Meestal wordt er een aantal weken gewacht en kijkt men hoe het been zich corrigeert over de volgende weken.
Indien er onvoldoende correctie is moet er een kleine chirurgische ingreep uitgevoerd worden die een periostale strip (sneetje in het botvlies) wordt genoemd (figuur 7).
Belangrijk is echter te weten dat het tijdstip voor deze correctie verschillend is van gewricht tot gewricht. De groeiplaat van het gewricht mag nog niet gesloten zijn.
Hieronder een tabel die aangeeft voor welke leeftijd een corrigerende behandeling moet uitgevoerd worden:

Bij milde vormen bestaat de behandeling enkel uit correctief bekappen en beslagen van de hoef.
Het correct bekappen en beslagen van de hoef moet om de 2-4 weken herhaald worden. Bij een X-been wordt de buitenzijde van de hoef wat ingekort zodat bij steunnname de binnenzijde van de hoef eerst op de grond komt. Bij een O-been wordt de binnenzijde van de hoef ingekort.
Deze veulens gaan best niet in de grote weide ter preventie van overbelasting van de groeiplaat. Indien het probleem niet opgelost is binnen de 4-6 weken is chirurgische ingreep misschien noodzakelijk.
De chirurgische behandeling bestaat uit:
Ofwel het been stimuleren in de groei, waar de groeiplaat te traag groeit (de ‘holle’ kant) doormidel van ‘periostale stripping’ of het insnijden van het botvlies (figuur 7).

Figuur 7: Een voorbeeld van periostale stripping. Hierbij wordt het botvlies ingesneden ter hoogte van de groeiplaat aan de kant die te traag groeit om de groei te stimuleren
Ofwel het been remmen in de groei waar de groeiplaat te snel groeit (de ‘bolle’ kant). Dit gebeurd door een schroef (figuur 8) of schroef en draadje (figuur 9) in of over de groeischijf te plaatsen.


Figuur 8: Op deze foto zien we dat er een schroef geplaatst is door de groeischijf van de voorknie aan de kant die te snel groeide om de groei te remmen
Figuur 9: Op deze foto zien we dat er 2 schroeven, verbonden door een draad, geplaatst zijn door de groeischijf van de voorknie aan de kant die te snel groeide om de groei te remmen
In erge gevallen wordt een combinatie van beide (periostale stripping in combinatie met een schroef of schroef met draad) uitgevoerd.
Grasvoet – bokvoet -klemvoet door retractie van de diepe buiger.

Figuur 10: Veulen dat op 2maand ouderdom plots op zijn teen begon te lopen links voor ten gevolge van een contractie van de diepe buigpees.
Bij een gras voet zit er een knik in de lijn tussen de kootbeenderen en de voorzijde van de hoefwand. De teen is te kort, de hiel te hoog. In erge gevallen loopt het paard nog enkel op de teen en raken de hielen zelfs de grond niet meer (figuur 10).
Milde gevallen worden behandeld doormiddel van een aangepast beslag dat meestal bestaat uit een ijzer met een verlegde teen en het inkorten van de hielen (figuur 11).

Figuur 11: Aangepast beslag met verlengde teen bij een veulen. De verlengde teen werkt als een hefboom en duwt de ingekorte hiel op de grond waarbij de diepe buigpees gerekt wordt.
Erge gevallen hebben een kleine bijkomende operatie nodig waarbij het check ligament onder de voorknie wordt doorgesneden. Dit geeft extra lengte aan de diepe buiger waardoor de hiel kan zakken. De operatie wordt steeds gevolgd door een revalidatie/stapschema gedurende een 2 tal maand.
Correctie treedt meestal op binnen de 2 maand na de operatie.
Naar voor knikken van de kogel door retractie van de buigers:

Figuur 12: Het naar voor knikken van de kogel links voor bij een jaarling met retractie van de buigpezen
Hier kan zowel de oppervlakkige als de diepe buigpees een rol spelen.
De kogel komt loodrecht op de grond te staan en bij erge gevallen knikt het veulen door de kogel naar voor toe (figuur 12).
Deze gevallen zijn ernstig en moeten snel behandeld worden. De chronische gevallen doen het minder goed na operatie.
De behandeling bestaat hier in een aangepast beslag samen met het doorsnijden van het check ligament van zowel de diepe als de oppervlakkige buiger.
Ook hier wordt de operatie gevolgd door een revalidatie/stapschema van ongeveer een 2 tal maand.
Correctie treedt ook hier best op binnen de 2 maand na de operatie zoniet wordt de kans op volledig herstel klein.
Conclusie
Het tijdig opmerken en aanpakken van een standafwijking zal de uitkomst van de behandeling aanzienlijk verbeteren. Neem contact op om correct advies te verkrijgen.
Paardendierenarts-Equine veterinarian Lucas Troch
The English version can be found below
My foal has a conformation defect: What now?
The foal season is in full swing again, and the first foals are happily frolicking in the pasture.
Every breeder hopes for a healthy and correctly built foal, but not all breeders are fortunate enough to have this luck. In some foals, the owner, farrier, and/or veterinarian notice something abnormal with the comformation of the hoof or the entire leg.
Timely detection of a deviation allows for quick correction if necessary. In case of doubt, the owner should contact the veterinarian to have the foal's leg stance checked and thereby apply the correct treatment.
Assessment of limb comformation in the foal
Assessing the stance of the limbs in the foal is best done on a hard, even surface. Here we observe the foal both standing still, attempting to position the foal as squarely as possible, and walking in a straight line (Figure 1).
Figure 1: Assessment of limb comformation in the stationary foal
In the stationary assessment, the foal is viewed from the front for the front legs and from the back for the hind legs. It is best to do this perpendicular to the front knee and hock respectively. This way, angular deformities (bowlegs or knock-knees) can be detected.
We look to see if an 'imaginary' straight line can be drawn through the middle of the hoof, fetlock, pastern, front knee/cannon bone, and upper leg. If this is the case, then there are no angular deformities present. If there is an angle in this 'imaginary' line, then it is referred to as varus (bowlegs, left horse in Figure 2) or valgus (knock-knees, right horse in Figure 2). Subsequently, radiographs can be used to determine the degree of deviation and whether surgical intervention is necessary.
Figure 2:
A sketch of a horse with bowlegs (left) and knock-knees (right)
The foal is assessed from the side to detect 'flexural' deformities (tendon retractions).
In 'flexural' deformities, the tendons are involved in the majority of cases. When the flexor tendons retract, the bone grows too quickly compared to the tendons, pulling the joint into flexion (Figure 3a). Hyperextension or excessive straightening of a joint usually occurs at birth due to laxity of the flexor tendons (Figure 3b).
Figure 3a: Foal that began to walk on its toe at 2 months of age due to contraction of the deep flexor tendon
Figure 3b: Pony foal that sinks through its fetlocks due to abnormal laxity (not strong enough) of its flexor tendons
Causes of limb deformities in foals
Simply put, the causes can be divided into 2 major groups:
1) Causes present before birth.
For example: abnormal positioning in the uterus, premature birth, uterine inflammation, mare's illness, hormonal or nutritional imbalance, incomplete bone ossification, etc.
In this case, the foal is born with the deformity.
2) Causes present after birth:
For example: unbalanced nutrition, growth plate trauma, pain (due to trauma, bruising, 'navicular syndrome', etc.) with secondary tendon retraction, rapid bone growth, growth plate infection, uneven load on the growth plate, growth plate overload, etc.
In this case, the limb deformities occur in the first 6 months after birth.
Types of limb deformities and their treatment
Bowlegs and knock-knees present from birth due to incomplete ossification of the bones of the front knee or hock:
In prematurely born foals, a bowleg or knock-knee may occur because the small bones in the front knee or hock are not sufficiently ossified (Figure 4B). The foal walks on these fragile bones, pressing them flat. This will cause an abnormal stance to develop.
Treatment consists of about 2 weeks of stall rest combined with splinting. Once there is sufficient ossification of these bones, the danger is averted.
The process of sufficient ossification is monitored by taking radiographs.
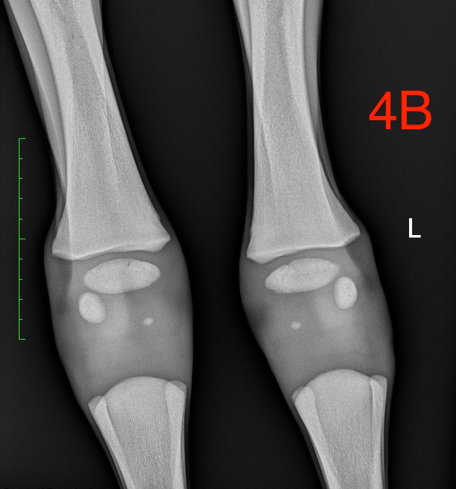
Figure 4A: A radiographic image of normal ossification of the bones of the front knee and Figure 4B a radiographic image of incomplete ossification of the bones of the front knee due to premature birth.
Another cause of bowlegs or knock-knees from birth is that some foals are born with a bowleg or knock-knee due to incorrect positioning in the uterus. These deformities usually disappear spontaneously within the first 4 weeks of life and do not require treatment.
Sinking through the fetlocks from birth:
Figure 5: Pony foal that sinks through its fetlocks due to abnormal laxity (not strong enough) of its flexor tendons
This problem occurs in newborn foals, especially in the fetlocks. They walk on the back of the fetlocks (Figure 5).
This involves laxity of the tendons and joint capsule, and in the majority of cases, the problem resolves itself over the following weeks as the foal grows and strengthens.
Treatment consists of rest in a large box and daily controlled movement (walking alongside the mare) for 15 minutes per day to strengthen the muscles and associated structures. Free-range turnout is initially not recommended as it can cause joint overload.
Bandages are not recommended in this case as they can worsen the situation.
Bowlegs and knock-knees that develop during foal growth:
Figure 6A: Left bowleg due to uneven growth at the level of the growth plate of the fetlock.
Figure 6B: Knock-knees on the left and right due to uneven growth at the level of the growth plate of the front knees.
These usually occur in the first weeks/month after birth, with knock-knees being more common than bowlegs.
Normally, the growth plate in a bone grows evenly along its entire length. However, in some foals, one side grows faster than the other. This can result in a bowleg (Figure 6A) or knock-knee (Figure 6B).
Heredity also plays a role here.
However, the bone has a mechanism to correct this uneven growth to some extent on its own. Surgery for a knock-knee is therefore not immediately necessary. Usually, a few weeks are waited, and then the leg is observed to see how it corrects over the next weeks.
If there is insufficient correction, a minor surgical procedure called periosteal stripping (a small incision in the bone membrane) may be performed (Figure 7).
However, it is important to know that the timing for this correction varies from joint to joint. The growth plate of the joint must not yet be closed.
Below is a table indicating the age at which corrective treatment should be performed:

For mild forms, treatment consists only of corrective trimming and shoeing of the hoof.
The correct trimming and shoeing of the hoof should be repeated every 2-4 weeks. In a knock-knee, the outside of the hoof is shortened so that when weight is applied, the inside of the hoof touches the ground first. In a bowleg, the inside of the hoof is shortened.
These foals are best kept out of the large pasture to prevent overload of the growth plate. If the problem is not resolved within 4-6 weeks, surgical intervention may be necessary.
Surgical treatment consists of:
Either stimulating growth in the leg, where the growth plate is growing too slowly (the 'concave' side) by means of 'periosteal stripping' or cutting the bone membrane (Figure 7).
Figure 7: An example of periosteal stripping. Here, the bone membrane is incised at the level of the growth plate on the side that is growing too slowly to stimulate growth.
Or slowing down growth in the leg where the growth plate is growing too fast (the 'convex' side). This is done by placing a screw (Figure 8) or screw and wire (Figure 9) in or over the growth plate.
Figure 8: In this photo, we see a screw placed through the growth plate of the front knee on the side that grew too quickly to slow down growth.
Figure 9: In this photo, we see two screws connected by a wire placed through the growth plate of the front knee on the side that grew too quickly to slow down growth.
In severe cases, a combination of both (periosteal stripping combined with a screw or screw with wire) is performed.
Grass foot - club foot - contracted foot due to retraction of the deep flexor.
Figure 10: Foal that began to walk on its toe at 2 months of age due to contraction of the deep flexor tendon.
In a club foot, there is a bend in the line between the pastern bones and the front of the hoof wall. The toe is too short, the heel too high. In severe cases, the horse walks only on the toe, and the heels do not even touch the ground (Figure 10).
Mild cases are treated with adapted shoeing, usually consisting of a shoe with an extended toe and shortening of the heels (Figure 11).
Figure 11: Adapted shoeing with extended toe in a foal. The extended toe acts as a lever and pushes the shortened heel to the ground, stretching the deep flexor tendon.
Severe cases require a minor additional surgery in which the check ligament under the front knee is cut. This adds extra length to the deep flexor, allowing the heel to drop. The surgery is always followed by a rehabilitation/walking schedule for about two months.
Correction usually occurs within two months after the surgery.
Forward knuckling of the fetlock due to retraction of the flexors:
Figure 12: Forward knuckling of the fetlock on the left in a yearling with retraction of the flexor tendons.
Here, both the superficial and deep flexor tendons can play a role.
The fetlock stands perpendicular to the ground, and in severe cases, the foal knuckles forward through the fetlock (Figure 12).
These cases are serious and must be treated promptly. Chronic cases do not do well after surgery.
Treatment here consists of adapted shoeing along with cutting the check ligament of both the deep and superficial flexors.
Here too, the surgery is followed by a rehabilitation/walking schedule of about two months.
Correction is also best within two months after the surgery; otherwise, the chance of complete recovery is small.
Conclusion
Timely detection and addressing of a conformation defect will significantly improve the treatment outcome. Contact for correct advice.
Equine Veterinarian Lucas Troch